Dietary Assessment Method: Analyzing How Sex and Gender Interact
Gendered Innovation 1: Analyzing Sex in Portion Size Increases Accuracy in Dietary Assessment
Method: Analyzing Sex
Method: Intersectional Approaches
Gendered Innovation 2: Understanding Gender Differences in Dietary Survey Completion Improves the Quality of Information.
Method: Analyzing Gender
Gendered Innovation 3: Gender-specific FFQs Perform Better in Validation and Analysis of Diet-Cancer Relationship
Method: Rethinking Concepts and Theories
Conclusions and Next Steps
The Challenge
Over the past several decades diet-related chronic diseases (DRCDs), including cancers and cardiovascular diseases, increased worldwide (World Health Organization, 2003). Understanding the relationship between dietary factors and DRCDs can lead to cost-effective and science-based disease prevention and management strategies.
Food Frequency Questionnaires (FFQs) are the most commonly used dietary assessment tool in nutritional epidemiological studies because they are cost-effective, easy to administer and are thought to give reasonable estimates of long-term usual intake—see figure below.
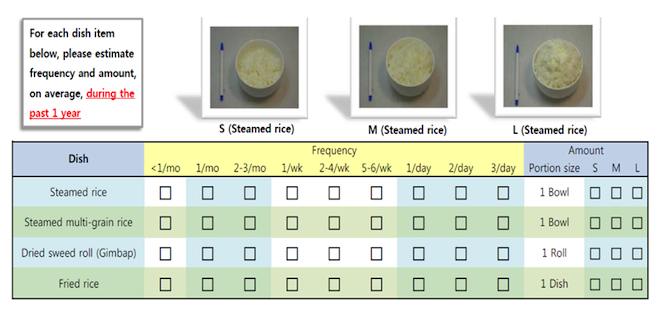
Example of a food frequency questionnaire (Modified from Park, 2011, 204)
Individual dietary intakes vary from day-to-day for many reasons, including age, socioeconomic background (food costs and availability), days of the week, food preference and behavioral factors (Beaton et al, 1979, 1983; Gwon et al, 2004; Willet, 2013). Sex and gender are also important diet-determining factors, but these have not been prospectively considered in the development, validation, and implementation of FFQs. Searching PubMed with various combinations of the keywords “FFQ,” “Food Frequency Questionnaire,” “Validation,” and “Validity” yielded 1,124 articles published between January 1983 and May 2014. Excluded were studies conducted in one sex or with subjects other than healthy adults, review articles, articles published in languages other than English, and articles that could not be found through web searches. The resulting 246 validation studies were examined to identify the development process of FFQs used in each study. Among them, only 148 articles described the development process of the FFQ. Since some FFQs were validated more than once, 48 studies that developed FFQs were identified for the remaining validation studies. Therefore, a total of 196 FFQ development studies were analyzed: only 21 studies (10.7%) were found to have considered sex in the development phase of FFQ. The sex of the survey subject was reported more often in determining portion sizes (7.7%) than in selecting food items or “dish” (5.6%). Among the 246 validation studies, only 36.6% reported the results by the sex—see chart below.
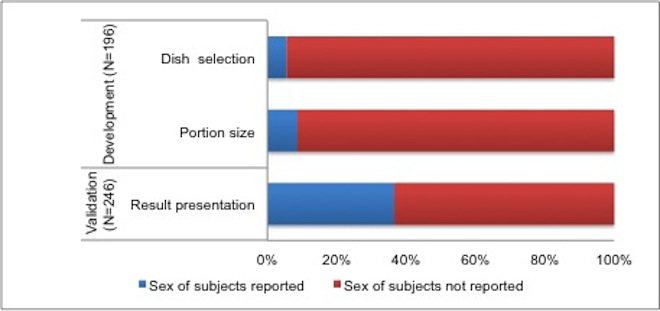
Sex of Subject Reported in the Development and Validation Studies of FFQs published between January 1983 and May 2014.
Gendered Innovation 1: Analyzing Sex in Portion Size Increases Accuracy in Dietary Assessment
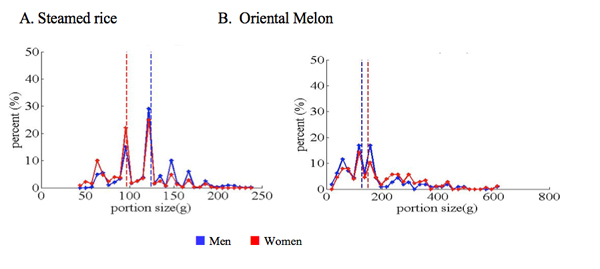
The Fourth Korean National Health and Nutrition Examination Survey (KNHANES IV) conducted 2007-2009 (Korea Centers for Disease Control and Prevention, 2010) revealed differences between men and women (over age 30 years) along two dimensions important in FFQ development: 1) portion size (influenced by sex), and 2) dish selection (influenced by gender). Analyzing portion size revealed that sex and gender interact: men usually eat larger portions of selected foods, such as steamed rice, a staple of Korean diet. Women, by contrast, chose to eat larger portions of fruits and vegetables, such as oriental melon—see figure below. Dishes consumed frequently also differed by gender (data not shown). These sex and gender differences will impact major sources of energy and nutrients.
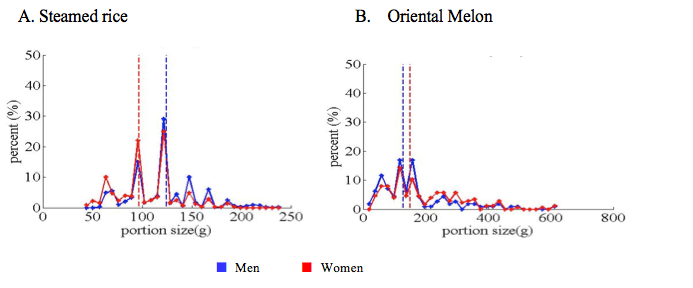
Distribution of portion sizes of selected dishes by sex. Men eat larger portions of rice; women eat larger portions of oriental melon. Data from the KNHANES IV 2007-2009 were reanalyzed.
Considering how sex and gender interact is important for identifying the association between diet and cancer. A dish-based FFQ was developed to study diet and cancer associations (Park et al., 2011). One-hundred and twelve dish items were selected considering the amount and frequency of consumption, contributions to energy, nutrients, and cancer-related dietary factors (CRDFs) suggested by the World Cancer Research Foundation (2007). Three portion sizes were assigned for each dish. When the portion size of each dish was re-evaluated by sex, portion sizes of 94 dishes (84%) differed significantly between men and women, 73% of the items were larger in men than in women (Noh et al, unpublished data). These results led to the development of sex-specific portion sizes for all items on the FFQ. A corrected FFQ was developed for each sex.
The original FFQ developed by Park et al. (2011) was validated in a study with 288 adults that consisted of 115 men and 173 women (50% more than men) against 12-day diet records collected over one year (Park et al., 2012). The dataset and the procedures were reexamined after correcting the portion sizes between men and women—while holding dishes available for selection constant.
Method: Analyzing Sex
FFQ validation data can be reevaluated retrospectively to analyze sex
- 1. Data are disaggregated by sex.
- 2. Dish items on FFQ are corrected for portion sizes for each sex.
- 3. Intakes of energy, macronutrients, and CRDFs are corrected for each sex.
- 4. Corrected data are compared to original data to yield a better understanding of dietary intakes.
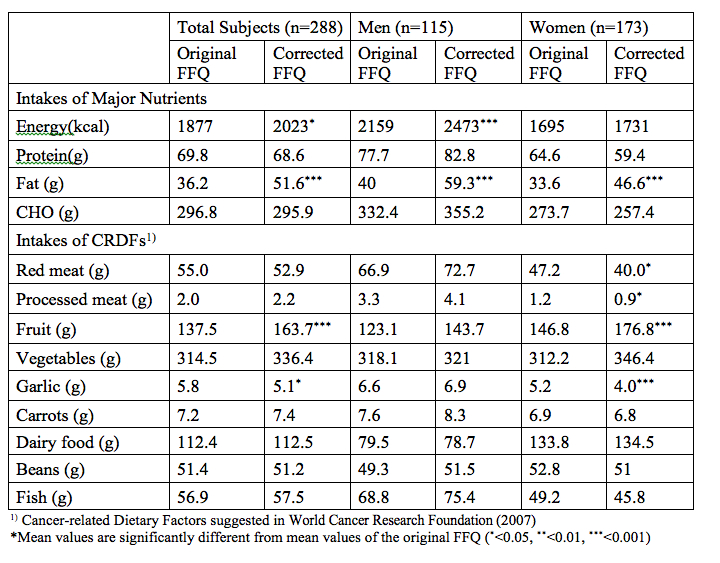
The results of the validation study were reevaluated after calculating intakes of each participant with the same consumption frequency but with the new sex-specific portion size. Energy intake calculated with corrected FFQ increased significantly in total subjects and men, while fat intakes increased significantly in both men and women (see table below; Noh et al, unpublished data). Correcting portion sizes by sex led to significant changes in CRDF-intake levels in women, but not in men. Analyzing portion size by sex sheds new light on important dietary factors including energy, fat, and cancer-related dietary factors. Importantly, aggregated data do not yield the true story for men or for women.
Mean Daily Intakes of Nutrients and CRDFs1) by the Original and Portion Size Corrected FFQs
Method: Intersectional Approaches
Other factors such as age, BMI, socioeconomic status (SES), and education affect diet and the effects may differ between men and women. Although women are considered more sensitive to social modeling of eating, a comprehensive review of the literature fails to support this hypothesis (Cruwys, et al, 2014). In a study of diet quality and BMI among Canadian adults (Sundararajan, et al, 2014), diet quality was negatively associated with BMI in high BMI group. The author noted that the association was stronger in women. Poorly educated elderly persons in the U.K. showed lower vegetable consumption in men but not in women. Financial hardship, on the other hand, decreased fruit consumption only in women (Conklin et al, 2014). Results of these studies indicate that effects of socioeconomic factors, education, BMI, and exercise on diet are heterogeneous in men and women.
Gendered Innovation 2: Understanding Gender Differences in Dietary Survey Completion Improves the Quality of Information.
Dietary assessments are conducted based on the assumption that responses to FFQs or any dietary assessment method are similar between men and women. In some cultures, men are less familiar with specific foods and cooking than women. Moreover, women and men’s eating practices, willingness to respond or familiarity with Likert-type scale, bubble format surveys differ. In societies where men do not cook or do not commonly complete questionnaires, they experience difficulties completing in dietary surveys.
Method: Analyzing Gender
- 1. Examine response rates for women and for men in dietary surveys by country.
- 2. Consider gender differences in familiarity with specific foods and cooking.
- 3. Develop FFQs that all participants can understand and answer.
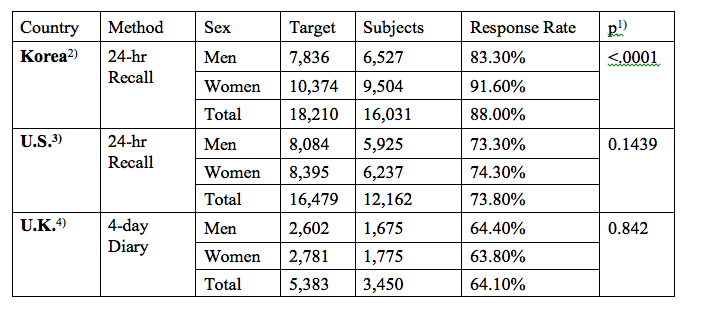
Response rates to national dietary surveys (among adults age 20 and over) differ by gender and country—see table below. Overall response rates in Korea are higher than in the U.S. and the U.K. Interestingly, the response rate of Korean women is much higher than that of Korean men in contrast to almost no difference between women and men in the U.S. and U.K. In order to minimize systematic errors due to differences in response rates between women and men at the national levels, sample weights are assigned for each respondent. Importantly, underrepresentation of men in a national database could lead to errors in selecting portion sizes and dishes when developing FFQs. Low response rates of one sex could also lead to errors in validation studies, as well as in epidemiological studies.
Response Rates of Adults Over 20 Years of Age in National Dietary Surveys
- 1) p from χ2 test
- 2) Korean Health and Nutrition Examination Survey Ⅳ (2007~2009). Information and data available from here
- 3) NHANES Survey 2007~2010 data combined. Information and data available from here
- 4) National Diet and Nutrition Survey Results from Years 1, 2, 3 and 4 (combined) of the Rolling Programme
(2008/2009 – 2011/2012); Information and data available from here
FFQs tend to be more difficult or cumbersome to complete than 24-hr recall (24HR) because subjects are asked to answer questions about usual food intakes over a longer period of time and the survey length is commonly over 100 items. Subjects’ responses are also limited to the list of food items provided and serving sizes given on FFQs; despite most FFQs asking open-ended response for “other foods consumed”, few respondents provide additional items in their response.
Subjects who were asked to complete FFQs reported more difficulties answering questions about multiple-item dishes than single dish items, and also more difficulty choosing a portion size than indicating consumption frequencies. In order to address the difficulties in completing FFQs, a qualitative cognitive interview survey was conducted with a FFQ developed by Ahn et al (2007). Among the five men and fifteen women who participated in the study, two men spent about 60 minutes completing the 103-item FFQ. The average length of time to complete the FFQ was 30.6 minutes for total subjects. Of note is the fact that none of the five men cooked at home while all 15 women reported being the main household cook. Several men in the study expressed difficulties understanding the pictures of some foods, and also the description of portion sizes (Lee et al., 2007).
The low response rates of subjects and differential response rates between women and men in dietary surveys (within countries) make it difficult to develop and administer FFQs equally valid for both gender. FFQs need to be designed so that all participants can fill them out with equal accuracy.
Gendered Innovation 3: Gender-specific FFQs Perform Better in Validation and Analysis of Diet-Cancer Relationship
Among the 196 FFQ development studies searched in the literature (see the Challenge section above), only 21(10.7%) developed FFQ with gender consideration. These FFQs are categorized as “Gender-specific FFQ” (GS-FFQ) and all others were categorized as “Not Gender-specific FFQ” (NGS-FFQ). The performances of FFQs of the two categories are examined in the validation studies and nutritional epidemiological studies on diet and colorectal cancer (Lee, 2015).
Method: Rethinking Concepts and Theories
- 1. FFQs are categorized by gender consideration in developmental phase.
- a. Gender-specific FFQ (GS-FFQ) if developed with gender analysis.
- b. Not gender-specific FFQ (NGS-FFQ) if developed without gender analysis.
- 2. Validation studies of FFQs in the two categories were identified and intakes of commonly reported nutrients were compared in relation to levels obtained by the reference method.
- 3. Meta-analyses were conducted for prospective cohort studies using GS-FFQs and NGS-FFQs to analyze effects of red meat intake and processed meat intake on colorectal cancer.
Gender-specific FFQs estimates dietary intake more precisely and with comparable accuracy in men and women. Of the 246 validation studies searched (see the Challenge section), only 45 (18.3%) studies used GS-FFQs. Among these studies, 46.7% reported the results by gender which is considerably higher than 33.3% reporting results by gender in studies using NGS-FFQs. Performances of FFQs in validation studies were examined by comparing intake levels for nutrients commonly reported in both groups—energy, carbohydrate, protein fat, cholesterol, fiber, and calcium. Mean ratios of intakes by FFQ to intakes by the reference method were almost identical for GS-FFQs (0.95 in men and 0.96 in women) but considerably far apart in studies with NGS-FFQs (1.00 in men and 1.12 in women). These results show that the accuracies of nutrient intake estimates are similar in both gender when GS-FFQs are used but significant overestimation of intakes in women may occur when NGS-FFQs are used. (Lee, 2015) The ability of GS-FFQs, compared to NGS-FFQs, to estimate dietary intakes of men and women with similar error have important implications for nutritional epidemiology.
Gender-specific FFQs Perform Better in Detecting the Association of Red Meat Intake and Colorectal Cancer.
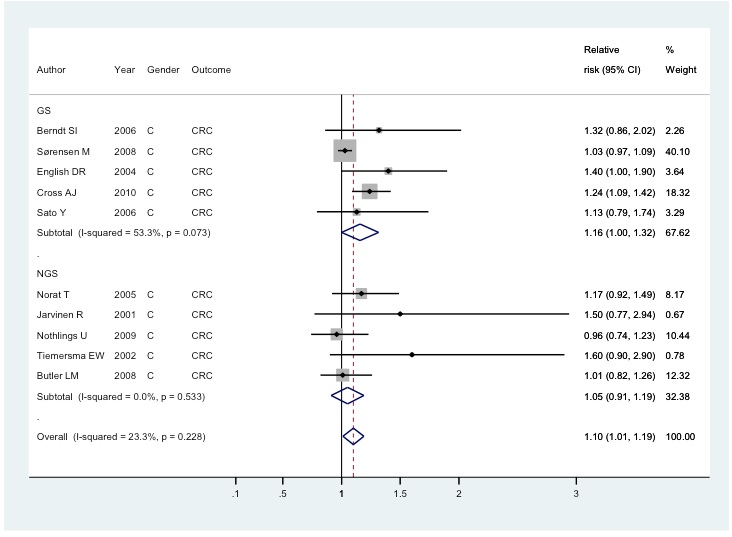
Lee (2015) examined the performance of GS-FFQ in detecting diet-disease relation. Of the 297 prospective cohort studies on diet and colorectal cancer selected by the World Cancer Research Foundation (2007, 2011), only 32 studies (10.8%) used GS-FFQs. Meta-analyses were conducted to estimate overall effects of red meat intake and processed meat intake on colorectal cancer. Ten prospective cohort studies that used GS-FFQ (n=5) and NGS-FFQ (n=5) showed an overall effect of red meat intake as a colon cancer risk factor (RR=1.10, 95% CI=1.01 to 1.19). This significance was apparent however only in studies with GS-FFQs (RR=1.16 95% CI=1.00 to 1.32) but not in studies with NGS-FFQ (RR=1.05, 95% CI=0.91 to 1.19)—see figure below.
Meta-analysis of studies reporting association between colorectal cancer and red meat intake selected by WCRF (2007, 2011). Studies in GS group used ‘Gender-specific FFQs’ and studies in NGS group used ‘Not gender- specific FFQs’ as described in Gendered Innovation 3 section.
Conclusions and Next Steps
Diet is an important factor for prevention and management of DRCDs. FFQs are a preferred tool for establishing and confirming diet-disease relationships. Sex is a critical determinant of the amount of foods consumed, and gender can influence the types of food consumed. Currently investigators working in nutritional epidemiology seldom consider sex and gender in the development and validation of FFQs. Correcting portion sizes for sex resulted in significantly new understandings of intakes for energy, nutrients and CRDFs with differential effects for men and women. Moreover, men more so than women tend to be underrepresented in dietary surveys and report more difficulties to answer to FFQs, particularly in societies where men do not engage in cooking. Limited evidences show that GS-FFQs perform better in validation studies and better in analyzing the association between red meat intake and colorectal cancer. It is critically important to recognize these gender challenges when developing, validating, and applying FFQs. Analyzing sex and gender, and how these interact, can lead to more accurate FFQs and thus ultimately better understandings of diet-disease relationships.
1. Gender-specific FFQs need to be developed for the list of preselected food items and respective portion sizes. Current FFQs should be evaluated in the context of gender and sex-specific constructs.
2. FFQs need to be developed, revised and validated periodically to reflect changes in dietary intake, eating behaviors and markets. While the prevalence of DRCDs are rapidly increasing worldwide, the resources for developing dietary assessment tools have been decreasing. It is crucial to secure proper resources for continuous updating dietary assessment tools.
3. FFQs should be simple to understand with special attentions given to men, especially in countries where they do not engage in daily cooking.
4. Validity of dietary assessment depends on complete and accurate food composition databases that include non-nutritive bioactive compounds in foods. Many newly identified bioactive components (such as caffeine, isoflavones, polyphenols, etc.) are of paramount importance in addressing general and gender specific diet-disease relations. Databases to estimate intake levels of these components are critically limited for epidemiological studies.
5. International cooperation for FFQ development and validation, together with expansion of food composition databases, is critically important in understanding diet-disease relation that may vary among countries with distinctive characteristics in diet and disease prevalence.
Works Cited
Ahn Y, Kwon E, Shim JE, Park MK, Joo Y, Kimm K, Park C, Kim DH. Validation and reproducibility of food frequency questionnaire for Korean genome epidemiologic study. Eur J Clin Nutr. 2007, 61(12), 1435-41.
Beaton GH, Milner J, Corey P, McGuire V, Cousins M, Stewart E, et al. Sources of variance in 24-hour dietary recall data: implications for nutrition study design and interpretation. Am J Clin Nutr. 1979, 32(12), 2546-59.
Beaton GH, Milner J, McGuire V, Feather TE, Little JA. Source of variance in 24-hour dietary recall data: implications for nutrition study design and interpretation. Carbohydrate sources, vitamins, and minerals. Am J Clin Nutr. 1983, 37(6), 986-95.
Berndt SI, Platz EA, Fallin MD, Thuita LW, Hoffman SC, Helzlsouer KJ. Genetic variation in the nucleotide excision repair pathway and colorectal cancer risk. Cancer Epidemiol Biomarkers Prev. 2006, 15(11) 2263-9.
Butler LM, Wang R, Koh WP, Yu MC. Prospective study of dietary patterns and colorectal cancer among Singapore Chinese. Br J Cancer. 2008, 99(9), 1511-6.
Conklin AI, Forouhi NG, Suhrcke M, Surtees P, Wareham NJ, Monsivais P. Variety more than quantity of fruit and vegetable intake varies by socioeconomic status and financial hardship. Findings from older adults in the EPIC cohort. Appetite. 2014, 83, 248-55.
Cross AJ, Ferrucci LM, Risch A, Graubard BI, Ward MH, Park Y, et al. A large prospective study of meat consumption and colorectal cancer risk: an investigation of potential mechanisms underlying this association. Cancer Res. 2010, 70(6), 2406-14.
Cruwys T, Bevelander KE, Hermans RC. Social modeling of eating: A review of when and why social influence affects food intake and choice. Appetite. 2015, 86, 3-18.
English DR, MacInnis RJ, Hodge AM, Hopper JL, Haydon AM, Giles GG. Red meat, chicken, and fish consumption and risk of colorectal cancer. Cancer Epidemiol Biomarkers Prev. 2004, 13(9), 1509-14.
Järvinen R, Knekt P, Hakulinen T, Rissanen H, Heliövaara M. Dietary fat, cholesterol and colorectal cancer in a prospective study. Br J Cancer. 2001, 85(3), 357-61.
Korea Centers for Disease Control and Prevention (2010). Korea Health Statistics 2009: Korea National Health and Nutrition Examination Survey (KNHANES IV).
Kwon ES, Ahn Y, Shim JE, Paik HY, Park C, Kimm K, Ju YS, Kim DH. Within- and between-individual variation in nutrient intakes with day of the week and season in Korean adults. Korean J Nutr. 2004, 37(10), 917-927.
Lee GS, Paik HY, Yi MS, Joung HJ. Response Experiences with a Semi-Quantitative Food Frequency Questionnaire: A Qualitative Study using Cognitive Interview. J of Nutr Health. 2007, 40(6), 566-575.
Lee H. Effect of gender-specific development on validation and utilization of food frequency questionnaire: a systematic review and meta-analysis. The Graduate School, Seoul National University, MS Thesis. 2015.
Lee, R. D. and Nieman, D. C. Nutritional assessment. Dubuque, IA, McGraw-Hill. 2015.
Noh H, Park MK, Kim J, Joung H, Paik HY. Reanalyzing sex/gender specific portion sizes for a dish-based food frequency questionnaire (DFFQ) affects estimation of dietary intake for Korean adults. (Unpublished Data)
Norat T, Bingham S, Ferrari P, Slimani N, Jenab M, Mazuir M, et al. Meat, fish, and colorectal cancer risk: the European Prospective Investigation into cancer and nutrition. J Natl Cancer Inst. 2005, 97(12), 906-16.
Nöthlings U, Hoffmann K, Bergmann MM, Boeing H. Fitting portion sizes in a self-administered food frequency questionnaire. J Nutr. 2007, 137(12), 2781-6.
Nöthlings U, Yamamoto JF, Wilkens LR, Murphy SP, Park SY, Henderson BE, et al. Meat and heterocyclic amine intake, smoking, NAT1 and NAT2 polymorphisms, and colorectal cancer risk in the multiethnic cohort study. Cancer Epidemiol Biomarkers Prev. 2009, 18(7), 2098-106.
Park MK. Development of Food Frequency Questionnaire and Assessment of Cancer-related Dietary Factors in Koreans. Ph.D. Dissertation. Graduate School. Seoul National University, Korea. 2011.
Park MK, Kim DW, Kim J, Park S, Joung H, Song WO, et al. Development of a dish-based, semi-quantitative FFQ for the Korean diet and cancer research using a database approach. Br J Nutr. 2011, 105(7), 1065-72.
Park MK, Noh HY, Song NY, Paik HY, Park S, Joung H, et al. Validity and reliability of a dish-based, semi-quantitative food frequency questionnaire for Korean diet and cancer research. Asian Pac J Cancer Prev. 2012, 13(2), 545-52.
Sato Y, Nakaya N, Kuriyama S, Nishino Y, Tsubono Y, Tsuji I. Meat consumption and risk of colorectal cancer in Japan: the Miyagi Cohort Study. Eur J Cancer Prev. 2006, 15(3), 211-8.
Subar AF, Thompson FE, Smith AF, Jobe JB, Ziegler RG, Potischman N, et al. Improving food frequency questionnaires: a qualitative approach using cognitive interviewing. J Am Diet Assoc. 1995, 95(7), 781-8; quiz 9-90.
Sundararajan K, Campbell MK, Choi YH, Sarma S. The relationship between diet quality and adult obesity: evidence from Canada. J Am Coll Nutr. 2014, 33(1),1-17.
Sørensen M, Autrup H, Olsen A, Tjønneland A, Overvad K, Raaschou-Nielsen O. Prospective study of NAT1 and NAT2 polymorphisms, tobacco smoking and meat consumption and risk of colorectal cancer. Cancer Lett. 2008, 266(2), 186-93.
Thompson FE, Subar AF, Brown CC, Smith AF, Sharbaugh CO, Jobe JB, et al. Cognitive research enhances accuracy of food frequency questionnaire reports: results of an experimental validation study. J Am Diet Assoc. 2002, 102(2), 212-25.
Tiemersma EW, Kampman E, Bueno de Mesquita HB, Bunschoten A, van Schothorst EM, Kok FJ, et al. Meat consumption, cigarette smoking, and genetic susceptibility in the etiology of colorectal cancer: results from a Dutch prospective study. Cancer Causes Control. 2002, 13(4), 383-93.
Tsubono Y, Kobayashi M, Takahashi T, Iwase Y, Iitoi Y, Akabane M, et al. Within- and between-person variations in portion sizes of foods consumed by the Japanese population. Nutr Cancer. 1997, 29(2), 140-5.
Willett, W. Nutritional epidemiology. Oxford, New York, Oxford University Press. 2013.
World Health Organization. Diet, nutrition and the prevention of chronic diseases. WHO Technical Report Series, No. 916 (TRS 916). 2003.
World Cancer Research Fund/American Institute for Cancer Research. Food, Nutrition, Physical Activity, and the Prevention of Cancer: a Global Perspective. Washington DC: AICR. 2007.
World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Report. Food, Nutrition, Physical Activity, and the Prevention of Colorectal Cancer 2011. Washington DC: AICR. 2011.
Dietary Assessment: Analyzing How Sex and Gender Interact In a Nutshell
Diet-related chronic disease is increasing worldwide. Sex and gender affect diet, but the vast majority of researchers do not consider these factors when creating and validating Food Frequency Questionnaires (FFQs), one of the most common tools to assess diet. Researchers in Korea have found that women and men often make difference choices about which foods to eat and in what amounts (Figure 1).
Gendered Innovations:
1. Correcting FFQs for differences between women's and men's choices of portion size and food items can improve dietary assessments.2. Understanding gender differences in dietary survey completion improves the quality of information. Completing FFQs has been reported to be difficult for men in cultures where they are not familiar with specific foods and cooking. Developing surveys understandable to all sectors of the population will help researchers better identify significant associations between diet and disease.
3. Gender-specific FFQs perform better in detecting the relationship between diet and certain types of cancer.